
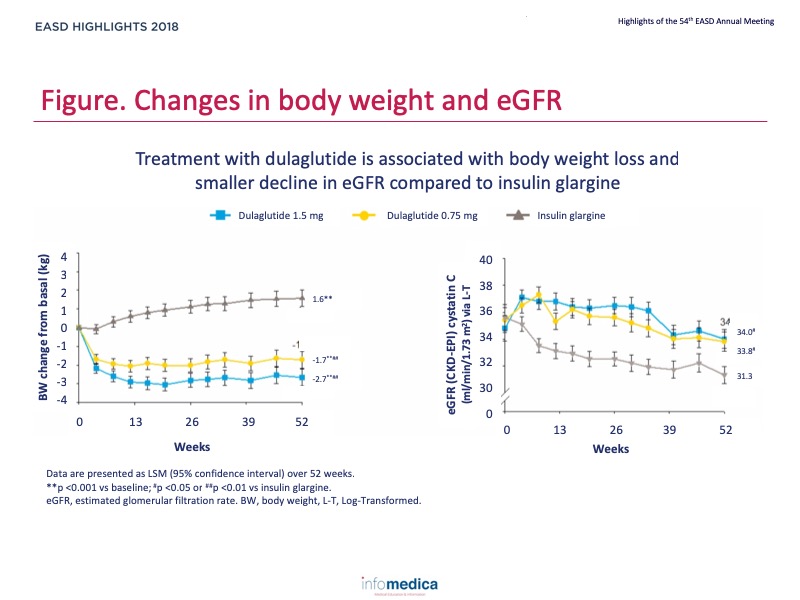
Many antihyperglycaemic drugs, including insulin, are primarily cleared by the kidneys, restricting treatment options for patients with kidney disease. Dulaglutide is a long-acting glucagon-like peptide-1 (GLP-1) receptor agonist that is not cleared by the kidneys, and confers a lower risk of hypoglycaemia than insulin. The AWARD-7 trial has shown that in patients with type 2 diabetes (T2D) and moderate-to-severe chronic kidney disease, once-weekly dulaglutide produced glycaemic control similar to that achieved with insulin glargine, with reduced decline in estimated glomerular filtration rate (eGFR) and significant weight loss.
Type of study, patients, and inclusion criteria
Patient population
Primary outcome measure
Secondary outcome measures
Main findings of AWARD-7
Main findings of the post-hoc analysis
Present disclosure: Katherine R. Tuttle has reported relationships with Eli Lilly, Boehringer Ingelheim, AstraZeneca, and Gilead.
Written by: Patrick Moore, PhD
Reviewed by: Marco Gallo, MD