
CARMELINA1 is a large, long-term cardiovascular (CV) outcomes trial testing the impact of linagliptin vs. placebo on top of standard care on CV and renal outcomes. The trial was designed to fulfil the linagliptin regulatory requirements for CV safety in a type 2 diabetes (T2D) population at high risk of CV risk enriched with chronic kidney disease (CKD). Based on its unique enriched CKD population, CARMELINA can add further evidence on the long-term safety of linagliptin on kidney function and heart failure.
Type of study, patients, and inclusion criteria
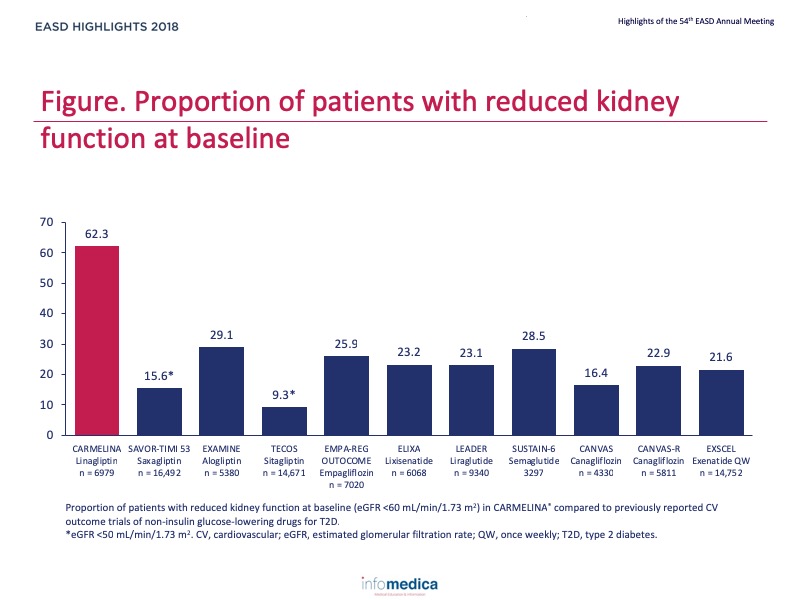
Patient population
Primary outcome measure
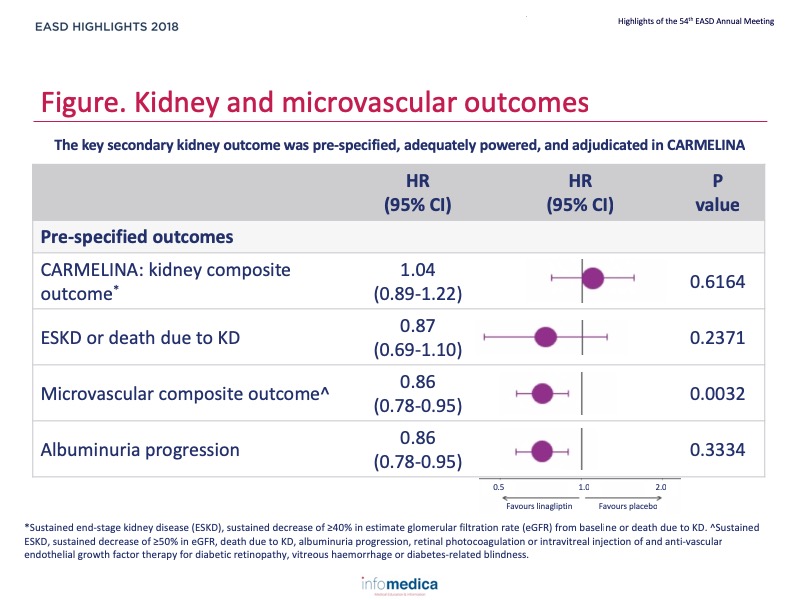
Secondary outcome measures
Baseline characteristics and metabolic endpoints
Cardiovascular outcomes
Renal outcomes
Hypoglycaemia and safety
Presenter disclosure: Julio Rosenstock has served on scientific advisory boards and receive honoraria or consulting fees from Eli Lilly, Sanofi, Novo Nordisk, Janssen, AstraZeneca, Boehringer Ingelheim, and Intarcia; he has also received grants/researcher support from Merck, Pfizer, Sanofi, Novo Nordisk, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Genetech, Janssen, Lexicon, Boehringer Ingelheim, and Intarcia.Robert Toto reports consultant fees from Amgen, Boehringer Ingelheim, ZS Pharma, Relypsa, Novo Nordisk, Reata, and AstraZeneca, and receives grant support from the NIH.Steven Kahn reports fees for advisory (advisory boards, steering committees) service to Boehringer Ingelheim, Elceylx, Intarcia, Janssen, Merck, Novo Nordisk.Darren McGuire reports clinical trial leadership for Merck AstraZeneca, Janssen, Eli Lilly, Boehringer Ingelheim, Novo Nordisk, Lexicon, Eisai, GlaxoSmithKline, Sanof Aventis; consultancy for Novo Nordisk, Boehringer Ingelheim, Eli Lilly, Merck, AstraZeneca, Metavant, Applied Therapeutics.Vlado Perkovic reports consults for Abbvie, Astellas, Bristol-Myers Squibb, Boehringer Ingelheim, Eli Lilly, GlaxoSmithKline, Janssen, Novartis, Retrophin, and AstraZeneca; has received lecture fees or grant support from Baxter, Boehringer Ingelheim, Merck, and Pfizer; and his institution has held clinical trial contracts with Abbvie, Roche, Janssen, Servier, and Novartis.Mark Cooper reports fee for advisory services from Boehringer Ingelheim.Bernard Zinman reports grant support from Boehringer Ingelheim, AstraZeneca, and Novo Noridsk; and consulting fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck, Novo Noridsk, and Sanofi Aventis.Philip D. Homes has reported that no relationships exist relevant to the contents of this presentation.
Written by: Patrick Moore, PhD
Reviewed by: Marco Gallo, MD