
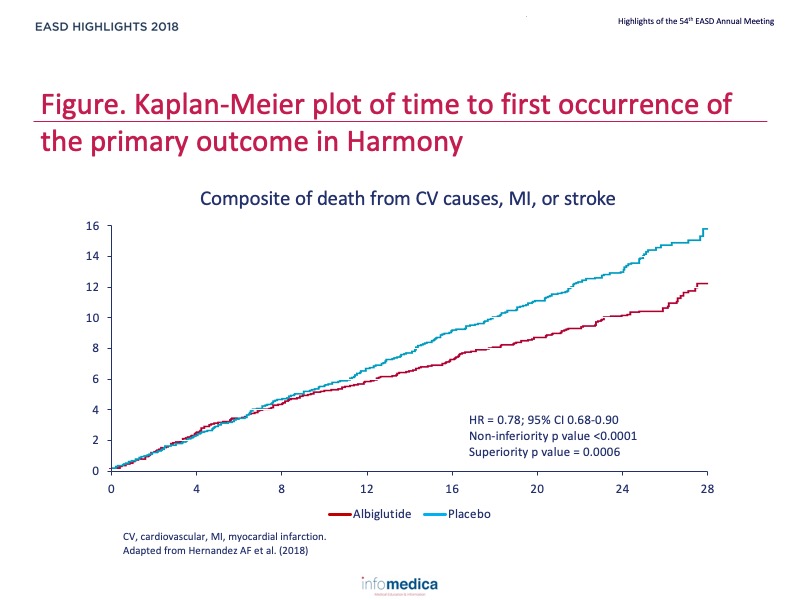
Glucagon-like peptide 1 receptor agonists differ in chemical structure, duration of action and their effects on clinical outcomes. The cardiovascular (CV) effects of once-weekly albiglutide in type 2 diabetes are not well characterised.
Type of study, patients, and inclusion criteria
Patient populations
Primary outcome measure
Secondary outcome measures
Primary endpoints or outcomes
Secondary endpoints or outcomes
Present disclosure: Adrian F. Hernandez reports grants to his institution from AstraZeneca, GlaxoSmithKline, Luitpold Pharmaceuticals, Novartis, Merck, Portola Pharmaceuticals, and Verily; and he has been a consultant for AstraZeneca, Bayer, Boehringer Ingelheim, Boston Scientific, Novartis, and Merck. Jennifer B. Green reports grants to her institution from AstraZeneca, Boehringer Ingelheim, and GlaxoSmithKline; and she has been consultant for AstraZeneca, Boehringer Ingelheim, Novo Nordisk, and Merck. SJ, NPJ, and KMT are GlaxoSmithKline employees and shareholders. Stefano Del Prato reports grants to his institution from AstraZeneca, Boehringer Ingelheim, Merck, and Novartis; he reports honoraria for presentations from AstraZeneca, Boehringer Ingelheim, Eli Lilly and Company, Merck, Novartis, Novo Nordisk, and Takeda Pharmaceuticals; and he reports participation in advisory boards for Abbott Laboratories, AstraZeneca, Boehringer Ingelheim, Eli Lilly and Company, GlaxoSmithKline, Merck, Mundipharma, Novartis Pharmaceuticals, Novo Nordisk, Sanofi, Servier, and Takeda Pharmaceuticals. John J.V. McMurray reports grants to his institution from Boehringer Ingelheim and Bristol-Myers Squibb, consultancy fees to his institution from Amgen, AstraZeneca, Bayer, Bristol-Myers Squibb, Cardurion Pharmaceuticals, DalCor Pharmaceuticals, GlaxoSmithKline, Johnson & Johnson, Merck, Novartis, and Theracos, and honoraria to his institution for presentations from AstraZeneca, Novartis, and Pfizer.
Christopher B. Granger reports grants to his institution from Apple, Armetheon, Daiichi Sankyo, the US Food and Drug Administration, and AstraZeneca; and reports consultancy fees from AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, GlaxoSmithKline, Janssen Pharmaceutica, Medtronic, the National Institutes of Health, Novartis, Pfizer, AbbVie, Boston Scientific, Gilead Sciences, Medscape, Merck, Novo Nordisk, Rho, Roche Diagnostics, Sirtex Medical, and Verseon.
Written by: Patrick Moore, PhD
Reviewed by: Marco Gallo, MD
Trial sponsor: GlaxoSmithKline Research & Development (GSK).
Trial: NCT02465515