
Des preuves solides suggèrent que l’apparition du diabète serait liée à un perte de fonction des cellules ß. Les interventions visant à réduire la masse adipeuse ou atténuer ses effets sur le métabolisme sont celles qui permettent de retarder et/ou de prévenir le diabète de type 2 avec le plus de succès (DT2).
Type of study, patients, and inclusion criteria
Patient population
Primary outcome measure
Secondary outcome measures
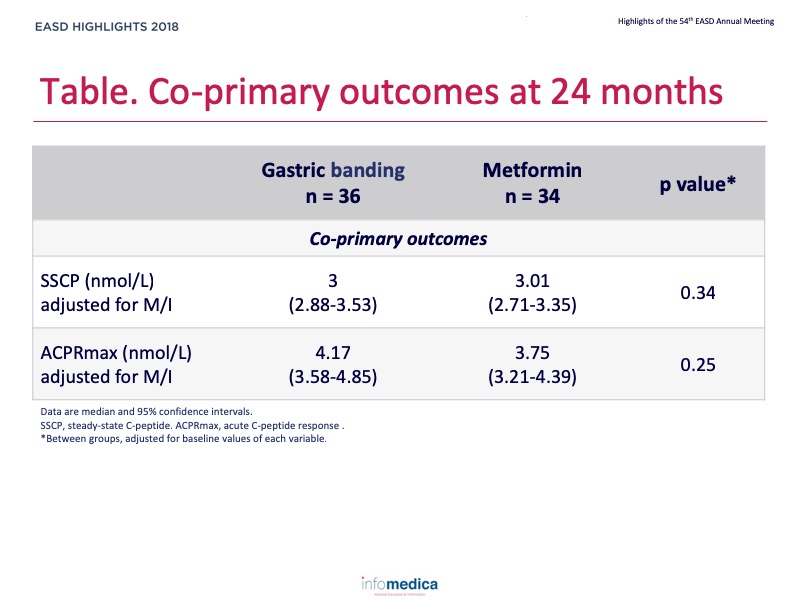
Primary endpoints or outcomes
Secondary endpoints or outcomes
Type of study, patients, and inclusion criteria
Patient population
Primary outcome measure
Secondary outcome measures
Primary endpoints or outcomes
Secondary endpoints or outcomes
Present disclosure: Anny H. Xiang has reported that no relationships exist relevant to the contents of this presentation. Thomas A. Buchanan has reported relationships for research support whit Allergan Corporation and Apollo Endosurgery.
Written by: Patrick Moore, PhD
Reviewed by: Marco Gallo, MD